
I’ve been revisiting the evidence of the early spread of the virus in 2019 and the first confirmed cases and I’ve arrived at what I think is the most likely course of events for how the virus emerged.
To cut a long(ish) story short, it looks like the virus was spreading globally by the second half of November 2019. The bit that was hard to understand was why, if it was in countries all round the world that winter, the explosive outbreaks only began in February and March 2020. Looking again at the reports of the emergence of the virus in close detail, it appears that this is because the virus’s journey from first emergence in autumn 2019 to explosive outbreaks in early 2020 occurred in a slower and more staggered way than we might expect from a simple understanding of viruses. This is not because the virus wasn’t present in countries prior to causing explosive outbreaks there – that’s the simplistic assumption that is contradicted by the data – but because the virus doesn’t always cause explosive outbreaks when it is present.
The novel SARS-like virus seems to have first started infecting humans around the end of October 2019. This was very likely in Wuhan. It might be suggested that if the virus was spreading globally in November 2019 then it could have started anywhere and the fact that it was first detected in Wuhan implies nothing about where it started. However, it does appear that the December outbreak in Wuhan where it was first detected was the largest to that date. In addition, the following month Wuhan was the first place to experience an explosive outbreak that taxed the health services, some weeks before anywhere else. The fact that it was ahead of the curve in these larger outbreaks is a strong indicator that the virus had been there longest and originally emerged there.
Molecular clock studies, which analyse the genetic make-up of early cases to calculate when their most recent common ancestor was around, tend to put the virus’s emergence in late October or early November, which is consistent with global spread towards the end of November.
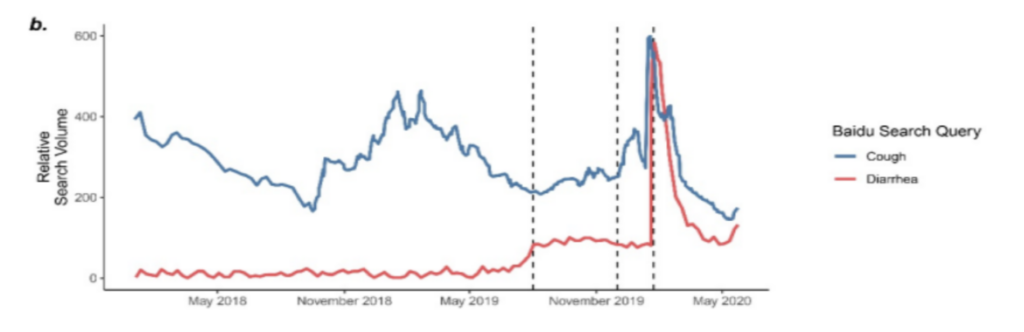
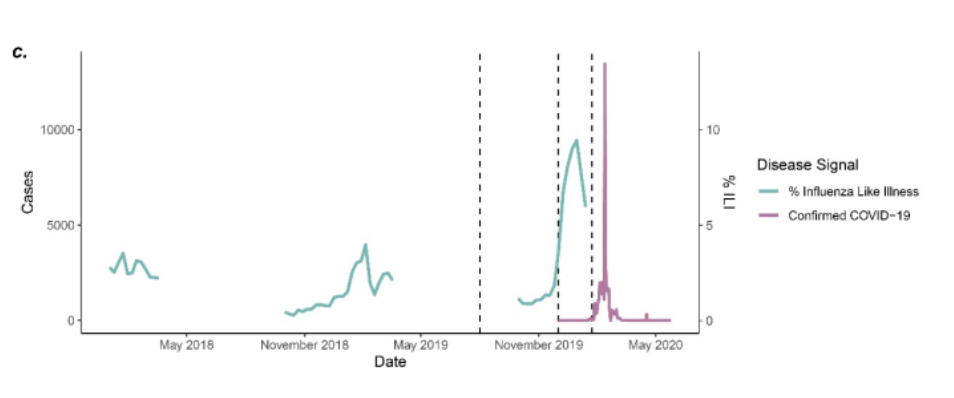
In China, a leaked Government report on early cases in Wuhan identified nine patients hospitalised in November 2019 with what was later confirmed as COVID-19 (the earliest symptom onset date was November 17th), though these have never been added to the official total. A study also claimed to find no neutralising antibodies in Wuhan blood donors in September to December 2019, though it’s unclear how reliable this is. ‘Baidu’ internet searches in Wuhan for ‘cough’ did not rise until December (see below, top) and likewise there is no spike in influenza-like hospital admissions until December (bottom).
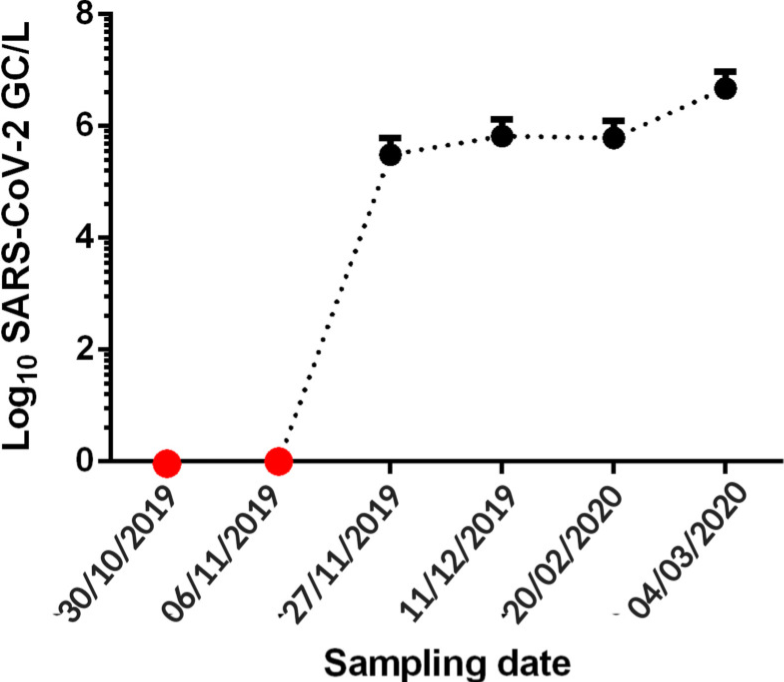
In Brazil, banked wastewater samples turned positive as of November 27th 2019, indicating significant community spread of SARS-CoV-2 at the end of the month. Interestingly, samples from Italy in a separate study didn’t turn positive until December 18th. No wastewater positives have turned up earlier than this anywhere (save for an anomalous positive for Barcelona in March 2019 that is widely believed to be a false positive).
In England, Imperial’s REACT study tested around 150,000 people for antibodies in early 2021 and asked those who tested positive when they recalled having symptoms. This resulted in the following graph.
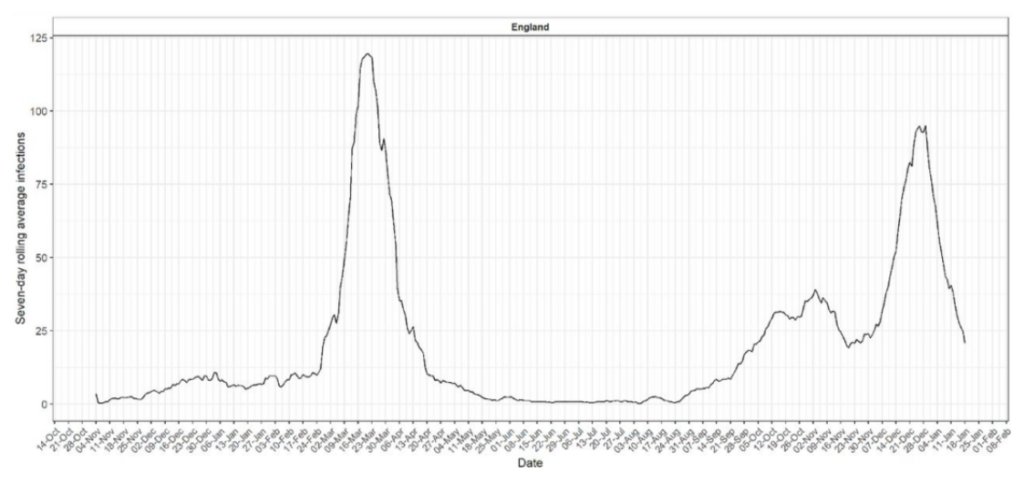
A notable rise in symptomatic illness can be seen from the end of November 2019 to a steady level that continues through the winter. The explosive outbreak of the first wave in late February 2020 is also clearly visible. This graph neatly illustrates how the virus can circulate for months at a low level (three months in this case), including through the winter flu season, before an explosive outbreak occurs, apparently out of the blue.
We don’t have good data from the United States on early spread as the country has consistently failed to undertake studies on stored samples of wastewater or from individuals, save for one Red Cross antibody study that found antibodies in mid-December 2019 but did not look at earlier samples or confirm with testing for viral RNA. Nonetheless, there has been no shortage of news reports from the U.S. that have told the stories of several individuals who became ill with Covid-like illness in November 2019 and later tested positive for Covid antibodies (when they had not been ill in the interim). These individuals include Michael Melham of New Jersey, who reports being infected along with several others at a conference around November 21st 2019; Uf Tukel, who reports being infected in Florida along with 10 others in late November 2019; Stephen Taylor and his wife, infected in Texas in November 2019; and Jim Rust, infected in Nebraska the same month. Bill Rice, Jr. has collected together the media stories of these early antibody-confirmed U.S. cases. It is notable that none of them claim to have been infected before November.
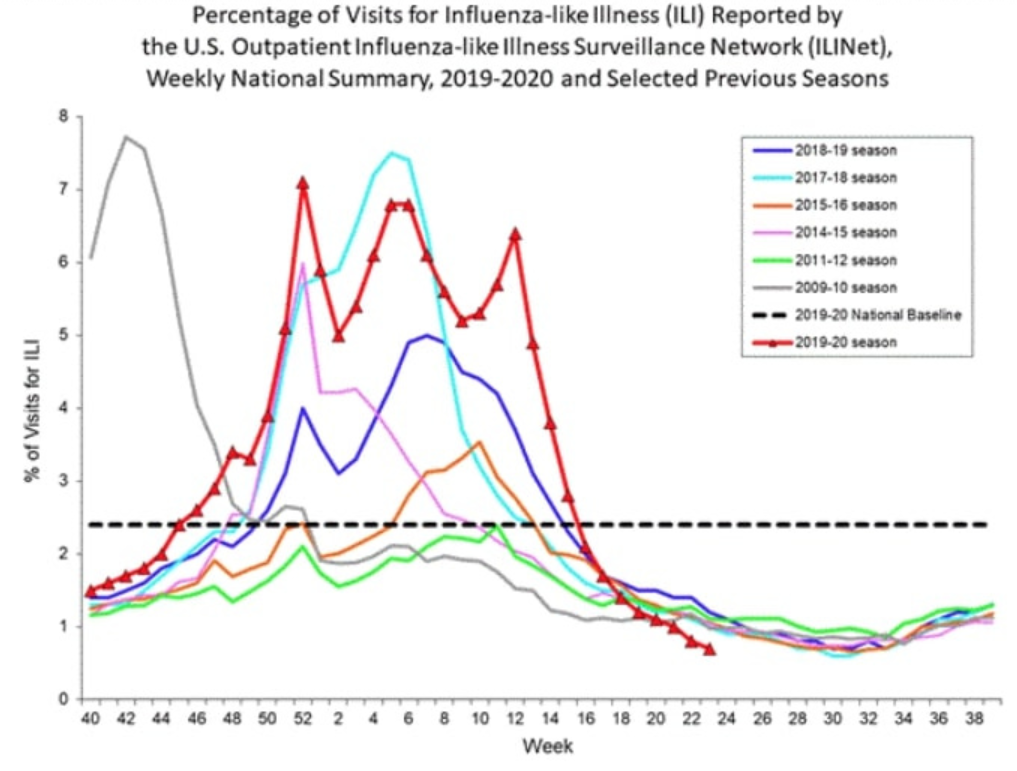
A chart of influenza-like illness incidence in the U.S. also shows no notable increase in symptomatic disease before November 2019 (see red line below; November is around weeks 44-48).
The evidence of late November spread in China, Brazil, England and America is, I think, highly persuasive; even if one or two of the cases turn out to be mistaken, I do not think it likely that all of them will be. They are also consistent with the estimates of the aforementioned molecular clock studies. This evidence suggests that the virus was not spreading globally much earlier than this. This is based on the negatives in the wastewater studies, the negligible levels in the Imperial study, the lack of Americans reporting illness, and the absence of patients in China. The studies which appear to show earlier global spread than this may be due to cross-reaction of antibodies or contamination of the high-magnification PCR testing.
This allows us to conclude that the virus was spreading at low level around the world by late November 2019, but probably not much earlier than this. What happened next?
The outbreak in the Huanan market appears to have begun around December 1st – this was the earliest symptom onset date in the first cluster of confirmed Covid patients, who began to be admitted to hospital on December 16th (note that a British teacher based in Wuhan who visited the market frequently reported falling ill on November 25th). This outbreak appears to have been significantly larger than other outbreaks up to that point. By January 2nd, 41 patients had been confirmed as admitted to hospital with a positive Covid test along with pneumonia and a characteristic chest CT scan; six of them later died. It was this cluster of hospitalisations that led to the detection of the virus, as at least nine samples from these patients were sent by clinicians for genomic analysis between December 24th and December 31st 2019. The detection of the virus in the wet market outbreak therefore appears to have been a direct consequence of the severity of that outbreak – it caused significantly more hospitalisations than other outbreaks up to then and prompted a number of clinicians independently to send samples for identification. This made it basically inevitable it would be detected during this outbreak.
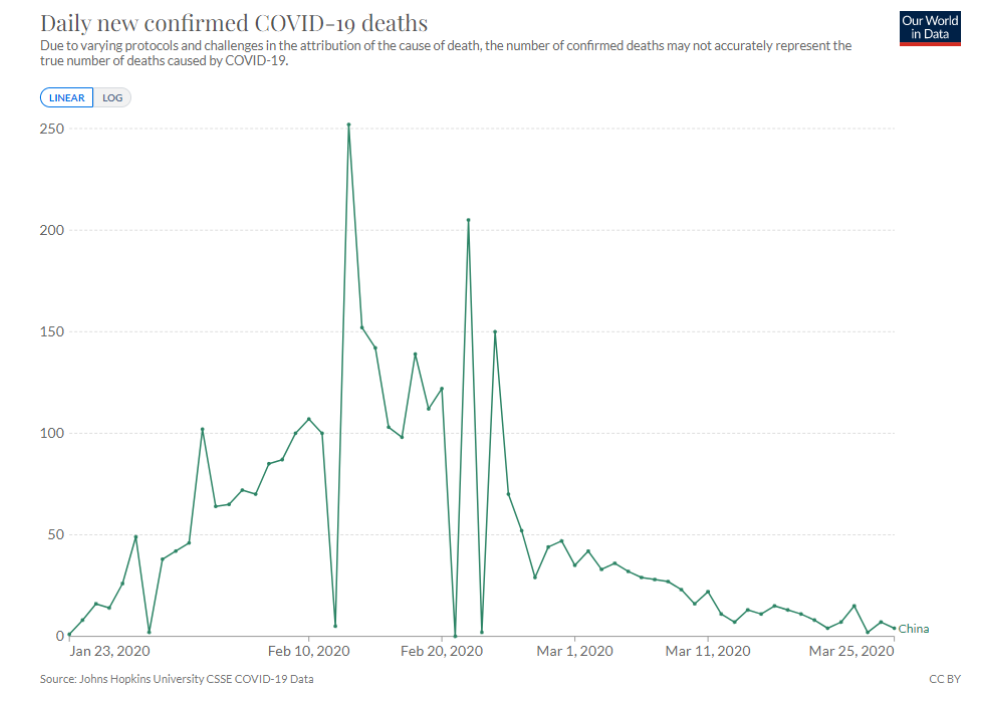
That said, the outbreak was very small compared to most of the waves we’ve seen since 2020, and indeed compared to what happened in China the following month. Looking at the curve of reported Covid deaths for China in 2020 indicates that the explosive outbreak in the region didn’t really begin until the first days of January (by counting back around 20 days).
This may explain why there was initial uncertainty about whether there was human-to-human transmission, while by January 14th it was becoming increasingly obvious that there was as they were in the middle of an explosive surge for the first time. It was also likely the recognition of this explosive outbreak that prompted the Chinese authorities to impose restrictions on Wuhan from January 23rd.
Oddly, the explosive January outbreak in Hubei province was not replicated in other parts of China, which were largely left untroubled by the virus at this point. Instead, the next place to see an explosive outbreak was South Korea, over a month later in February, and once again it was oddly limited largely to one city, Daegu. It was on a similar scale to the Wuhan outbreak with a similar number of deaths.
Next it was the turn of Italy and Iran to experience explosive outbreaks, beginning in mid-February. The outbreak in Italy was still mainly restricted to one part of the country, though the scale of it was beyond anything yet seen, and the Iranian outbreak was of a similar magnitude. Then followed New York and the north eastern United States, and also England, France and much of Western Europe (though not Eastern Europe or much of the rest of the U.S.). All these outbreaks were much closer to the larger Italian scale than the Chinese and South Korean scale. Other places continued with low level spread until they had their first explosive waves later in 2020, or in some cases in 2021 or even 2022.
What strikes me about this is how the size and scope of the outbreaks increased stepwise between November 2019 and February 2020. Spread in November 2019 was global but low level. In December, the Wuhan wet market outbreak took things up a notch, resulting in a higher number of hospitalisations and thus detection of the virus. Then in January, Wuhan experienced the first explosive Covid outbreak and wave of deaths. And in February the large European and American waves began, ramping up the scale another several notches, where it largely remained. (Omicron, when it came along in late 2021, boosted the size of outbreaks even further but considerably cut the death rate.)
This provides, I believe, a clear picture of how the virus emerged – via a stepwise move towards larger and larger outbreaks from an inauspicious start of low level spread in November. This movement is, I presume, largely a result of genetic changes in the virus, which alter its transmissibility in different populations and contexts – a hypothesis which is echoed by the authors of one major molecular clock study: “It is reasonable to postulate that the variant of SARS-CoV-2 that first emerged was less fit than the variant that spread through China and that evolutionary adaptation was critical to its establishment in humans.”
We can therefore, I think, be reasonably confident the virus first emerged in Wuhan during autumn 2019 and wasn’t just first detected there, as Wuhan was first to experience the larger outbreaks in both December and January, which suggests the virus had been there the longest.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Whilst I applaud what seem like Mr Dingwall’s good intentions, I am once again left underwhelmed at the calibre of the thinking of people that advise the government.
There is absolutely nothing wrong with doing things without evidence and not applying the precautionary principle BUT only when individuals are left to make their choices.
There is no instance where I would accept coercion by the state as acceptable, but if there is going to be any coercion, of course the precautionary principle must apply.
it just stuns me that the thinking of a government adviser, and presumably a highly educated man, can be so completely muddled and fails to make a critical distinction between forced collective action and free choice.
The world advances on adventurous innovation. That is precisely how entrepreneurs operate. And it’s fine as long as people are free to make their choices.
Let people grow GMO crops and let those who want to try them try them. Just don’t force anyone to consume them, keep the state’s heavy fingers off the scales and let people make their choices.
We don’t want a centrally planned society run by cautious bureaucrats. We want a free society, thanks very much.
I largely agree with you Stewart with the exception of:
“Let people grow GMO crops and let those who want to try them try them. Just don’t force anyone to consume them…”
Nope. There are enough problems being created in this world by rogue scientists as it is. The last thing we should be doing is giving them the nod to keep buggering about with nature. Fraudci would have a field day.
GMO is cod science and has NO place on this planet.
The crook Fauci. After the gain of function research scandal, I tend to agree. Besides there is plenty of resources without it. Ethiopia in the 1980s wasn’t because of a lack of food, but rather an engineered failure of distribution logistics (remind you of anything?).
Thanks Hugh.
As Michael Schellenberger points out in his book ‘Apocalypse Never’ the planet can feed everybody, the problems are caused by failures of distribution.
Indeed, recklessly tinkering with the genetic code itself to create novel organisms that could never have possibly existed otherwise? What could possibly go wrong?
Mother Nature really does NOT like to be effed with!
Spot on TSoAP.
The following is anecdotical but sounds plausible to me: The commercially mainly interesting thing about GMO crops is – hahaha – that they can be patented. Further, once they’re actually grown somewhere, the patented gene sequences will eventually migrate (via crosspollination) to the original, unmodified species, thereby enabling more royalty extraction as even farmers who didn’t originally grow GMO crops are now liable for patent infringement.
Gene engineering in any shape, size or colour is still nothing but a solution desparately in search of a problem, no matter if it’s applied to plants, viruses or vaccines.
You’ve reminded me of the chatter I’m hearing online atm about how these mRNA injections are effectively mutating people into becoming a different species and do they become the chattel property of whoever owns the patent for this nanotech? Katherine Watt, a paralegal and writer, wrote this piece about it. Sounds extremely far-fetched but it’s interesting;
… “On the legal side, homo borgiensis relates to the June 13, 2013 US Supreme Court ruling in Association for Molecular Pathology et al v. Myriad Genetics Inc.
In the Myriad case, SCOTUS affirmed that genetically-altered living organisms become the legal property of the holders of the gene-tech patents used to do the alteration. For the mRNA/DNA/nanotech injections, the patent holders are some combination of US government/Department of Defense and globalist pharmaceutical corporations.”
https://canadahealthalliance.org/wp-content/uploads/2022/10/Homo-borg-genesis_borgiensis-by-Katherine-Watt.pdf
That’s something very much different: GMO crops have their genome altered in order to grow into becoming somewhat different kinds of plans than the species they originally were. As (most) plants reproduces sexually, just with the help of pollen carrier species (insects), these genetically modified plants than have sex (so to say) with unmodified ones and the outcome is a cross of the modified and unmodified plant. That’s a real problem and it implies that even people (farmers growing corn) in the USA who didn’t originally use Monsanto corn end up having to pay royalties to the company. That’s the interesting effect of GMO crops. Anything beyond that is just window dressing to talk people into growing Monsanto corn.
The active ingredient in the so-called mRNA vaccines is just an artificially designed, defective virus (defective because it can’t reprogram cells to create complete copies of it). That’s bad enough, especially given the more than dubious benefits of them, because it means This injection is supposed to kill your cells (indirectly, by marking them as targets for elimination by T-cells). As usual for anything-COVID, the direct effects are known and intended to be harmful. And to which degree the indirect effects claimed to exist are actually beneficial is anybody’s guess.
Indeed, it’s actually and correctly called genetic pollution.
All I can say is let’s hope Pfizer tries to claim property over everyone that has had a Pfizer mRNA injection.
I think that would be too much even for the sheeple.
I triple dog dare them….
They sort-of already did that: As the nice theory goes, everybody who ever had a Pfizer injection is supposed to need another every three to six months until his death. That’s a form of serfdom: You’re required to put in a certain amount work and endure a little hardship to contribute to keeping the Pfizer franchise (still a very telling term) profitable.
Would I become chattel if subjected to spike protein shed?
“The commercially mainly interesting thing about GMO crops is – hahaha – that they can be patented.”
This is actually just what that world famous and genuine saint, saviour of humanity, Lord Bill of the Gates of Hell is doing.
India is one of his initial laboratories. Genuinely heritage seeds are effectively being stolen by Billy Boy goons, taken back to his labs for a bit of GMO monkey business and then sold back to farmers on the basis they increase yields, which they don’t.
The process is horrific. For the farmers.
Along with Bayer-Monsatan, et al.
Correct.
https://off-guardian.org/2022/11/03/indias-gmos-a-30-year-pathway-to-food-tyranny/
Indeed. Monsatan’s ultimate dream.
Here you go:
https://off-guardian.org/2022/11/03/indias-gmos-a-30-year-pathway-to-food-tyranny/
Politicians, bureaucrats and their advisers and experts etc. aka ‘the deep state’ are all ideologues, interventionists, zealous regulators of the plebs and power lusting control freaks benefitting directly from and all-in on that, now corporatist, system.
Their fear of loss of control correlates with their hubristic conviction that something is doable and will be successful- hence their ever more crazy and harmful policies, advise and actions and, above all, their tech-drunkenness, as well as their total inability to accept reality when it runs counter to their convictions and to apologize or change course then.
Sadly, that has also now led to the situation that Freedom has to be protected and often even regained from them and as such from our current, by them badly abused, mutilated and now clearly only fake, democracies.
But how and by whom?!
The sheep.
The wolves.
The sheepdogs.
Choose your poison.
So we just allow any whacko scientist to try whatever they like, encouraged by a system without rules, and hope that balance of potential benefit/harm is communicated fairly and equally to the general population, so everyone can do their research and make an informed choice? Yep, that’ll definitely work.
Except there were no “emergency conditions”, unless he’s speaking generally here. The best thing to do if evidence is absent is to do nothing. Adhere to the flipping WHO pandemic flu guidelines from 2019 that got thrown out of the window. Behave as we did every winter that we’ve all managed to survive by virtue of having a functional immune system.
But this is all moot isn’t it, and regurgitating the same old words, stressing the same tedious points over and over changes nothing. We all know now why most of the world ditched their pandemic preparedness plans and followed China ( land of communist psychopaths who revel in terrorising and dehumanising their citizens ) and became the WHOs bitches. They needed the scamdemic to generate fear and abusive restrictions to dehumanise and control so we’d be eager enough to take an untested, novel pseudo-vaccine. Anything to just get back to normal. And the muppets all fell for this utter crapola, hook, line and sinker. Talk about a social experiment..🤯😖
The made up coronavirus crisis is not the problem it’s the symptom.
It’s the symptom of decades of erosion of the idea of individualism and free choice and the ascendancy of a collectivist, centrally planned order, geared to solve made up and engineered problems.
The solution the person who wrote this article offers is to be very very careful with the central planning decisions. It doesn’t seem to occur to him that the solution is to just let people figure out how much risk they want to take in their lives and make their own decisions.
I don’t need any pandemic plan, good or bad, to be made and executed. I’m fine thanks.
If left to themselves, people will quickly figure out whether they are at risk or not and what to do if they think they are. And if there are dangers, in the market place of solutions the best will win out. It will certainly lead to better outcomes than some technocrat, bureaucrats micro managing the lives of 68 million people, just in this country.
Yes I agree. I’ve never sought guidance from authority, let alone the government, to decide for me if I’m fit and well enough to go into work or leave the house. To outsource your decision-making and allow the diktats of bureaucrats to trump your own common sense is just idiotic in my opinion. The only people who would do that are the people who completely fell for the PsyOp. They would have functioned perfectly fine using their autonomy until 2020 and then were manipulated into becoming mere automatons. It was pathetic, but famous experiments, such as Ash and Milgrim, ( not to mention the rise of the Nazi party ) have shown us repeatedly just how much of a push-over and highly malleable people are.
A fine comment Mogs. 👌
Seconded.
There were emergency conditions in care homes after the criminal government restrictions. But perhaps after all that was the point, to reduce demand for care-homes by putting people off (and maybe by killing some of the residents) in order to reduce the costs…
BINGO
Perhaps, but it’s far more likely that officials and medics made stupid decisions through panic, really badly thought out policy left unquestioned, hive-mindedness and circular reasoning.
Sedatives in a dose likely to be fatal for the elderly were recommended in ‘Covid end of life’ guidelines resembling the Liverpool Care Pathway (still available from various NHS trusts online), but one of the main side effects of midazolam and morphine is respiratory depression.
Very likely a substantial number of people had developed pneumonia as a result of infection (not necessarily just from Covid) and the decision was made – with no clinical evidence available outside of a hospital critical care ward – to ease their suffering. Some might have gone on to die from pneumonia, but it’s likely we’ll never know how many others might have survived. This would at least explain the vastly disproportionate number of people who died in hospitals and care homes, and the sudden, steep step change in the IFR with age.
Indeed, truly following the precautionary principle would be to follow the time-tested 2019 pandemic flu guidelines, and eschew any sort of lockdowns, quarantines, closures, masks, or novel experimental gene therapy “vaccines”.
“Pandemic policies would have looked very different if the precautionary principle had been applied correctly, especially to non-pharmaceutical interventions”
Sorry but exactly the same applies in spades to the pharmaceutical & medical interventions – the “vaccines” that are nothing of the sort, paxlovid which seems to make you iller, ventilators.
“Emergency conditions do not justify the abandonment of the precautionary principle.”
There was no emergency.
BANG!
“If action is urgent, but benefits and harms are uncertain, then the actions or innovations must be temporary, provisional and closely monitored with a view to withdrawing or halting them if their benefits are not proportionate to their harms.”
You’re living in a fantasy world if you think politicians, “experts” and “public health” officials will introduce stuff under the guise of “urgency” then withdraw it when they find it doesn’t work. They will double down. What % of covid lockdown and vaccine fanatics have admitted they were wrong? 1%?
ANY coercion is off the table, regardless of “urgency”. It has to be morally and it has to be practically because if it’s regarded as sometimes justified then it will be used sooner or later, as it has been with covid.
If action was urgent then the rational course would have been to encourage doctors to treat their patients with combinations of cheap and safe existing treatments and share the results, rather than wait several months for “vaccines” the longer term consequences of which couldn’t possibly be known, even if the trials had been carried out by conscientious, non-corrupt proper scientists.
Instead, people were effectively told to bugger off, only come back if they thought they were about to die, then be put on ventilators to make sure they did.
The government and health authorities couldn’t possibly have known that no existing treatments would help. However, they did know that effective treatments would prevent emergency use authorisation for the experimental gunks.
This was very clearly always about jabbing as many people as possible as many times as possible, not about protecting them from a virus that was known to pose a trivial threat to most.
And if the gunk jabs aren’t about protecting people from the trivial virus, what are they about? I can’t think of a benign explanation
“And if the gunk jabs aren’t about protecting people from the trivial virus, what are they about? I can’t think of a benign explanation.”
There is no benign explanation.
“Depopulation?”
Don’t be silly. Tssch, that’s one of those silly conspiracy thingies.
The term ‘precautionary principle’ is in the same category as ‘sustainability’, ‘global climate’, ‘theory’, ‘equity’, ‘diversity’, ‘intersectional’ and the rest. They mean only what the politically driven buffoons uttering them want them to mean – no more, no less.
The only difference between these and any other variety of common or garden horseshit is they are imbued with a moral weight through false conceptual association, intended to protect those who wield them from any scrutiny and providing them with a rhetorical cudgel to beat the impressionable into submission.
“The only difference between these and any other variety of common or garden horseshit is they are imbued with a moral weight through false conceptual association.”
Tip o’ the hat.
Just as Humpty Dumpty said to Alice
” It tells the advocates for innovation that they have to look just as hard for harms as for benefits.”
Whilst I believe in forgiveness, I also believe that those who failed to look for harms as well as benefits (i.e. a thorough cost-benefit analysis) with regard to the lockdowns shambles and experimental “covid” medication should be properly held to account (which by the way clearly includes the anti-truther Times muppets).
Could you not inject a bit more venom Hugh?
The precautionary principle is simply a fancy version of “first, do no harm” with some “look before you leap” thrown in for good measure. Until the Covidians turned it on its head to mean the complete opposite of what it originally meant, that is.
Reading through this article, I immediately thought “primum no nocere”.
Half way through the article the concept is discussed.
As a doctor who started training 42 years ago, this principle was instilled into my cohort from day 1.
It seemed sound, philosophically at the time, and nothing has caused me to change my mind on that.
To have that principle essentially consigned to the rubbish bin by technocrats and politicians, then have the majority of the profession offer no resistance, has been the most egregious part of the whole Covid debacle to my mind.
Thanks Dr G.
Dr G, thank you for this. Like you I cannot believe the medical profession offered no challenges to ‘The Science’. Given that evidence based medicine is still a thing; what can be the explanation?
Oh, they understand perfectly well what The Precautionary Principle is: They applied it zealously and enthusiastically during Covid … to existing off-patent medicines with stellar safety records.
Is Dr. Dingwall saying that his advice as explained in this article was over-ridden or was it not given at the time? It seems there are many people who claim to have been against almost all of the failed drugs and restrictions during Covid, so how did we finish up in the mess we are in now? Is it because leaders of governments ignored this advice or are poor badly science educated to understand it. It seems to me that politicians in general are poorly educated in what really matters in the world to be allowed to control people’s lives. We need to grade politicians by at least a minimum level of scientific knowledge, which Maggie Thatcher had, but none of our PM’s since have had. Perhaps that is why they have all been so useless.
Doing things without evidence though is often not just a case of acting “just in case”. It is often because governments cannot wait for evidence which may take years or never come at all, in their determination to put public policy in place. A good example is “climate change” where the precautionary principle is used where they always talk of the risk of using fossil fuels. But what they never do is talk about the risks of not using them, and since 90% of the worlds energy comes from fossil fuels, that risk is huge. The precautionary principle is used in one way only in order to justify preferred policies. Doing this kind of thing can lead to serious unintended consequences. On the issue of climate, it has led to huge sums of money diverted to turbines, solar panels, and all manner of assorted save the planet schemes costing hundreds of billions that could have been put to better use, and we wouldn’t be coerced into getting rid of energy that works and is cost effective. We are currently about to spend between one and two trillion eg on NET ZERO. If the assumptions that the precautionary principle is based on are wrong or not nearly as serious as anticipated then we will have squandered vast sums for no good reason. But then the politicians will say that they were only “listening to the scientists” and acting “just in case”. —A cautionary tale