Dr. Richard Ennos, a retired Professor of Evolutionary Biology at Edinburgh University, has undertaken a thorough analysis of the U.K.’s COVID-19 ‘Yellow Card’ vaccine adverse event data and found it indicates “unequivocal safety signals” for adverse reactions caused by the Pfizer and Moderna vaccines affecting the blood, the heart and female reproduction. He concludes that: “There can be no question that the mRNA vaccines should be withdrawn with immediate effect.”
In the U.K., three COVID-19 vaccines – AstraZeneca (AZ), Pfizer (PF) and Moderna (MO) – have been used in a nationwide inoculation programme aimed at preventing harm from the SARS-CoV-2 virus. All three vaccines provide the genetic code that enables vaccinees to produce within their bodies the spike protein of the SARS-CoV-2 virus, the molecule associated with the pathology of COVID-19. In the AZ vaccine the genetic code for the spike protein takes the form of DNA, and is introduced into recipient’s cells by a genetically modified chimpanzee virus (DNA, adenovirus vector). For the PF and MO vaccines, the introduced genetic code takes the form of heavily modified RNA, and is carried to recipient’s cells within lipid nanoparticles (mRNA, lipid nanoparticle). There is no control over either the tissues to which the vaccines are transported or the length of time for which spike proteins are produced by those tissues.
All three vaccines rely on novel technology that has never before been used in humans. At the time of their introduction, they lacked any long-term safety data, and therefore required Conditional Marketing Authorisation from the Medicines and Healthcare products Regulatory Agency (MHRA). To monitor the safety of the three vaccines the MHRA established the COVID-19 vaccine Yellow Card reporting scheme (C-19VYC). This collates standardised reports of suspected adverse reactions to the COVID-19 vaccines that can be analysed to detect safety signals and potentially trigger withdrawal of the vaccines. Here we show that a thorough analysis of the C-19YC data indicates unequivocal safety signals for adverse reactions caused by the mRNA vaccines PF and MO affecting the lymph system, the heart and female reproduction.
The strength of the C-19VYC reporting scheme is that it is capable of generating an enormous amount of valuable information about adverse reactions to the experimental COVID-19 vaccines. Reports of suspected adverse reactions can be submitted not only by physicians but also by the recipients of the vaccines themselves, providing valuable feedback to the MHRA based on first-hand experience. This inclusive aspect of the C-19VYC reporting scheme has proved very successful, with nearly half a million adverse event reports submitted, roughly one for every hundred recipients of the COVID-19 vaccines in the U.K.
Despite this strength in terms of quantity of data, the C-19VYC reporting scheme has a number of serious weaknesses related to the nature of the data collected. These weaknesses place limits on the scheme’s ability both to detect and to measure safety signals. The first problem is that the scheme does not identify or include a control group of individuals, who have not taken the vaccine, against which to compare those who have. Other major weaknesses are that reporting is passive rather than planned and takes place at a single point in time. Thus, reporting relies on the sufferer of the adverse reactions or his or her physician making the connection between the vaccine treatment and the adverse reaction. As a consequence, many adverse events will go unrecorded, and this becomes more likely the longer the delay between treatment and the associated adverse reaction. Reporting rates of adverse reactions are also likely to represent only a fraction of actual cases because physicians or recipients may have too little time to fill out the onerous paperwork, may not have knowledge of the Yellow Card scheme, or may be unwilling to countenance the idea of harms resulting from a medication in which they have placed trust.
As well as being low, reporting rates are expected to vary substantially between different sectors of the population. Experience shows that females post roughly three times more adverse event reports than males, and the reporting rate for adverse reactions varies with age, dropping off in the elderly population where adverse reactions may be obscured by multiple forms of pre-existing chronic illnesses. In addition, reporting rates are likely to vary with the severity of the adverse reaction. Individuals are far more likely to have the motivation and tenacity to file a report if their adverse reaction is severe than if it is mild. On the other hand, if the adverse event results in death, grieving friends or relatives may be too preoccupied to file a C-19VYC report.
Recognising the limitations in the C-19VYC programme is a very necessary first step in exploiting the enormous volumes of data that it has produced. In its published summaries the MHRA is at pains to emphasise that the Yellow Card data cannot be used to calculate true rates of adverse effects or to compare the safety of the different vaccines, both because of the nature of the data and the existence of many confounding factors. I view the MHRA’s statements as a challenge. In the remainder of this article, I will endeavour to show that the MHRA’s view is overly pessimistic and that the enormous efforts of those who have submitted Yellow Card reports of COVID-19 vaccine adverse effects have not been in vain.
In order to independently analyse the C-19VYC reports, it is essential to have access to the raw data. The first FOI request for access to the full anonymised C-19VYC data was made in June 2021. This, and subsequent FOI requests have been refused on the grounds that it would be too onerous to pass on the raw data, and that anyway the data would be published at a future date. However, it should be noted that the MHRA sends the C-19VYC data without delay to the companies that market the COVID-19 vaccines. Some 18 months after the first FOI request, the MHRA has at last released information gathered by the C-19YC scheme that is sufficiently detailed to allow independent analysis and calculation of safety signals.
A cursory look at the C-19VYC data indicates that the rate of reporting of serious and fatal adverse events is nearly three times higher for the adenovirus AZ vaccine (3.912 serious or fatal reaction reports per 1,000 doses) than for either of the mRNA vaccines PF or MO (1.341 and 1.344 serious or fatal reaction reports per 1,000 doses respectively). Although there has been no formal withdrawal of the AZ vaccine by the MHRA, the use of the AZ vaccine has effectively been discontinued, perhaps because of this worrying safety signal. With the discontinuation of the AZ vaccine, the most important question becomes whether serious safety signals can be detected for the remaining mRNA COVID-19 vaccines, PF and MO, that are still being employed.
As I have emphasised earlier, the data available from the Yellow Card scheme are the result of passive reporting. This means that any detailed analyses based on absolute numbers of reports of adverse reactions are problematic. However, a well-established protocol, known as proportional reporting rate analysis (PRR) has been devised for detecting safety signals using passive reporting data such as those collected by the C-19VYC scheme. The principles underlying the PRR protocol are explained below.
Suppose that we wish to see whether a novel vaccine substantially increases the frequency of a particular adverse reaction, say severe headache. If there is no connection between administration of the vaccine and the frequency of severe headaches, then the proportion of all adverse reaction reports that are severe headache should be the same for the novel vaccine as for the established and thoroughly tested vaccines. However, if administration of the novel vaccine does cause severe headaches, there will be a higher proportion of all adverse reaction reports that mention severe headaches for the novel vaccine than for the established vaccines. By dividing the proportion of adverse events which mention severe headache in the novel vaccine by this same proportion calculated for the established vaccines, we obtain a measure of the strength of the safety signal for severe headaches caused by the novel vaccine, the proportional reporting rate or PRR.
A safety signal is formally detected if three conditions are met. First, there must be a substantial number of reports of the chosen adverse reaction in the novel vaccine database. Second, the proportion of all reports that mention the chosen adverse reaction must be statistically significantly greater for the novel vaccine than for the established vaccines. This can be established using a simple ‘chi squared’ test. Thirdly, the proportion of adverse reactions calculated for the novel vaccine must be at least twice that calculated for the established vaccines (PRR>2).
To apply this PRR methodology to detect safety signals for the novel mRNA COVID-19 vaccines PF and MO, we make the very conservative assumption that the AZ vaccine does not increase the frequency of the particular adverse reactions that we are investigating. The AZ vaccine thus takes on the role of the safe, established vaccine in the PRR analysis. Therefore, we use data from the AZ vaccine to calculate the proportion of the chosen adverse events that we would expect in an established, safe vaccine. We then calculate the proportions of the chosen adverse event reports that occur in the PF and MO data, and compare these with the figure that we have calculated for AZ to obtain the PRR. If there is a significantly higher proportion of the chosen adverse event reports in the mRNA vaccines than in the AZ vaccine, and the PRR for the mRNA vaccine is two or more, this constitutes a strong safety signal requiring investigation and appropriate action.
In December 2022, MHRA released two data files from the C-19VYC scheme for each of the three COVID-19 vaccines. The first file contains an identifier for each Yellow Card report, the sex and age of the individual involved, and a classification of the severity of his or her adverse reaction – non-serious, serious or fatal. The second dataset includes the report identifier and various medical classifications of the adverse events suffered (there may be more than one adverse event per report). Perhaps the most accessible classification for the layman is based on the tissue type affected by the adverse reaction e.g. muscle, nerve, blood. By marrying up the two datasets, it is possible to create a single file for each of the COVID-19 vaccines that includes the report identifier, the sex and age of the patient, the tissue type affected by the first adverse event listed in the report (to avoid pseudo-replication of the reports), and the severity of the adverse reaction.
Data in the file described above are used here for PRR analysis to detect and measure the strength of safety signals associated with the adverse effects of the mRNA vaccines PF and MO on blood (harm to the blood and lymph system), the cardiac system (harm to the heart), and reproduction in females (harm to the menstrual cycle). The analysis has been confined to severe adverse reactions (serious plus fatal) to avoid the possible charge that the adverse reactions we are analysing are of little consequence to those they affect. To acknowledge the fact that reporting rates vary with both age and sex, the reported PRR values have been calculated in samples that are matched for both age and sex. This allows vulnerability to particular adverse reactions to be compared between age groups, and between females and males. It should be noted that when the analysis is conducted in the manner described, it yields minimum estimates of the strength of the safety signals because it assumes that the AZ vaccine does not increase the rate of the adverse reaction being studied. If this is not the case, the estimated strength of the safety signal associated with the mRNA vaccine concerned will be greater than we report.
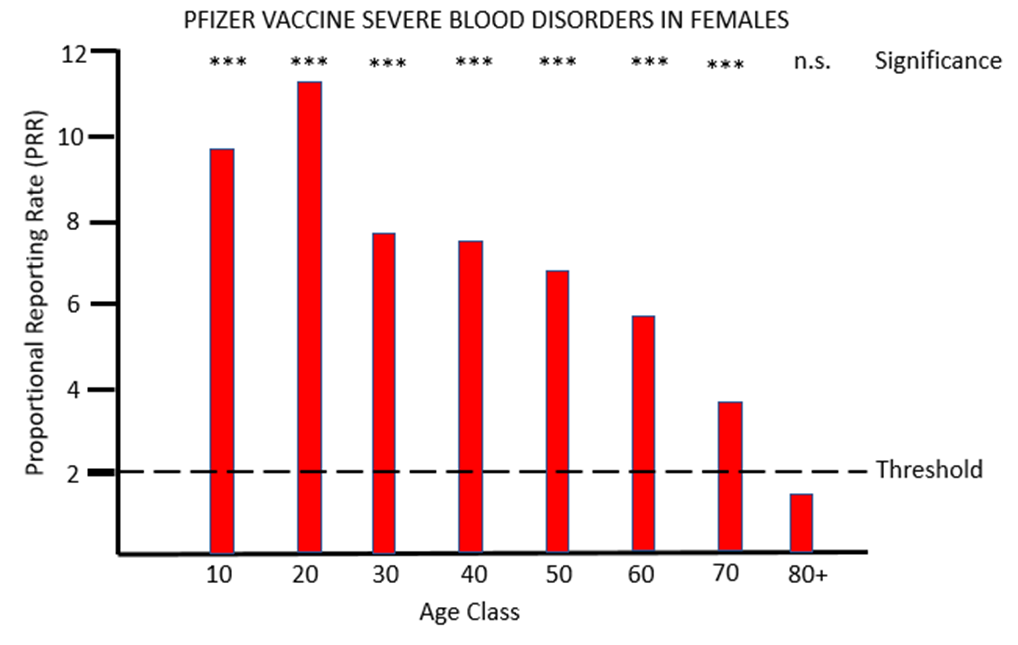
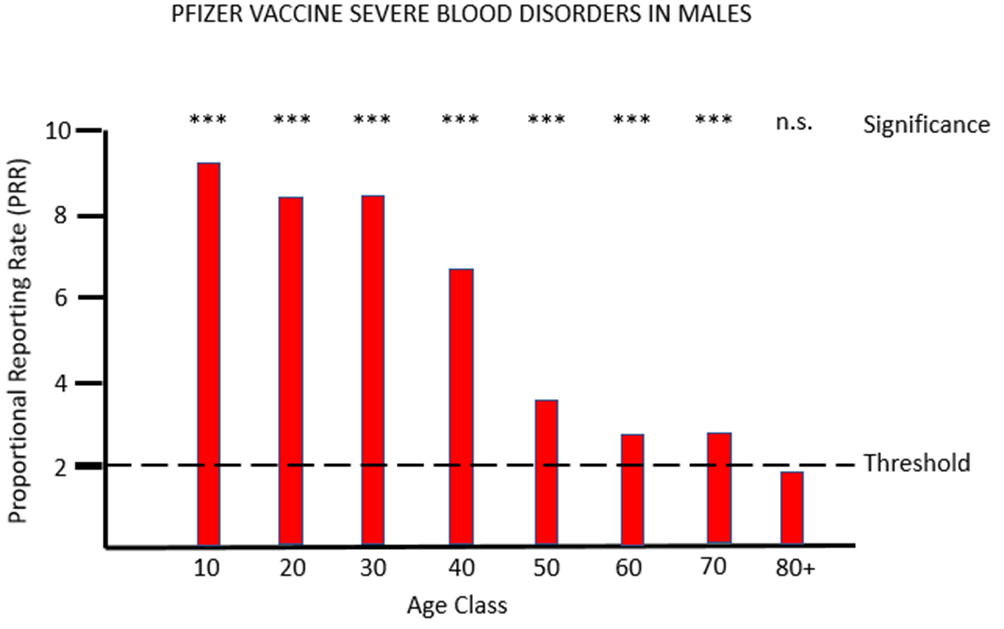
Figure 1a and 1b show the results for females and males respectively of PRR analysis of adverse reactions associated with the PF vaccine that affects tissues grouped under the MHRA classification blood (blood and lymph systems). For both sexes, and across all except the very oldest age class, there are very striking safety signals, with proportions of severe adverse event often more than eight times higher after PF vaccination than after AZ vaccination.
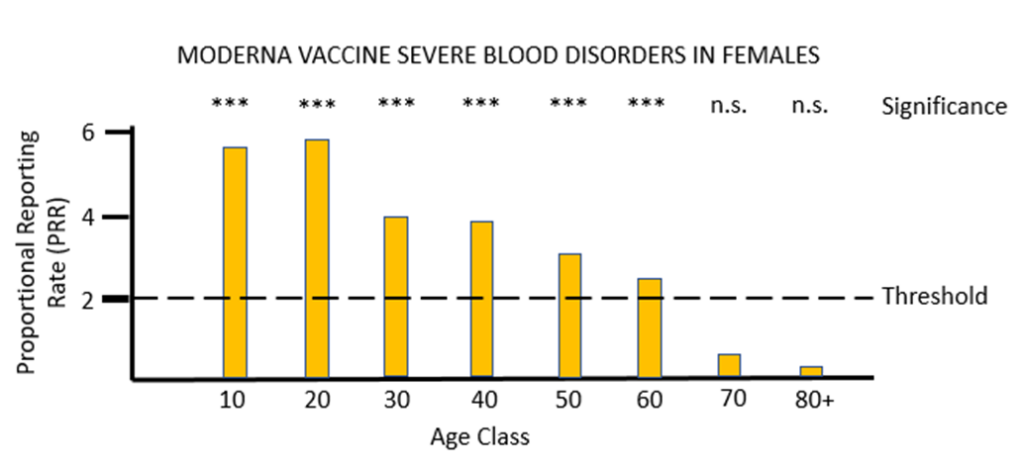
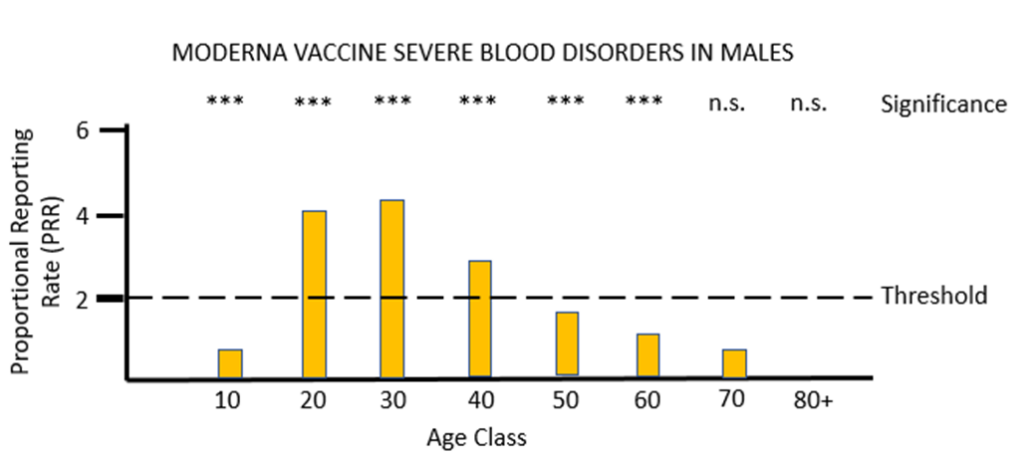
For the other mRNA vaccine MO, the proportional reporting rate is again very significant and well over the threshold level for safety signals in most of the female age classes and in males aged between 20 and 49. The vast majority of these severe adverse reactions affect the lymph system rather than the blood, and the diagnosis given is lymphadenopathy. It is very worrying that in its “Coronavirus vaccine – summary of Yellow Card reporting” in January 2023 the MHRA fail to mention any possible adverse effects of the mRNA vaccines on the lymph system, despite such a strong safety signal being present when the Yellow Card data are appropriately analysed.
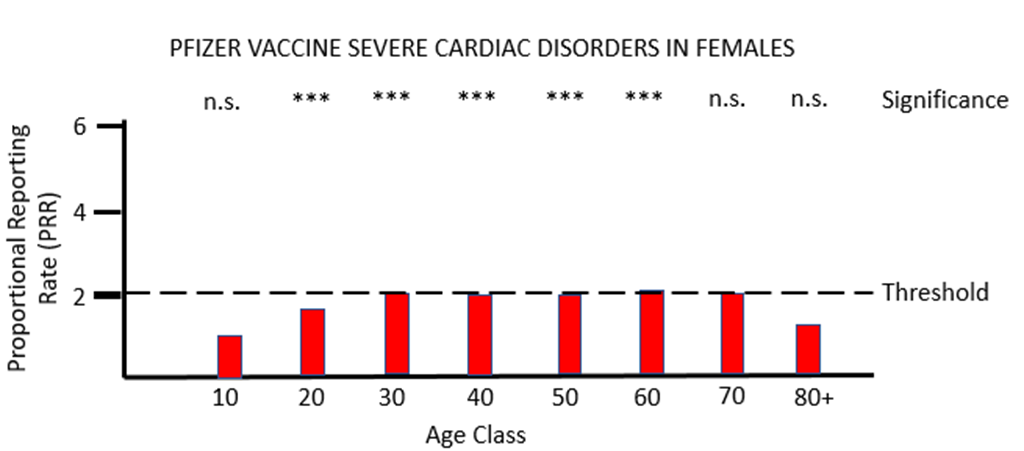
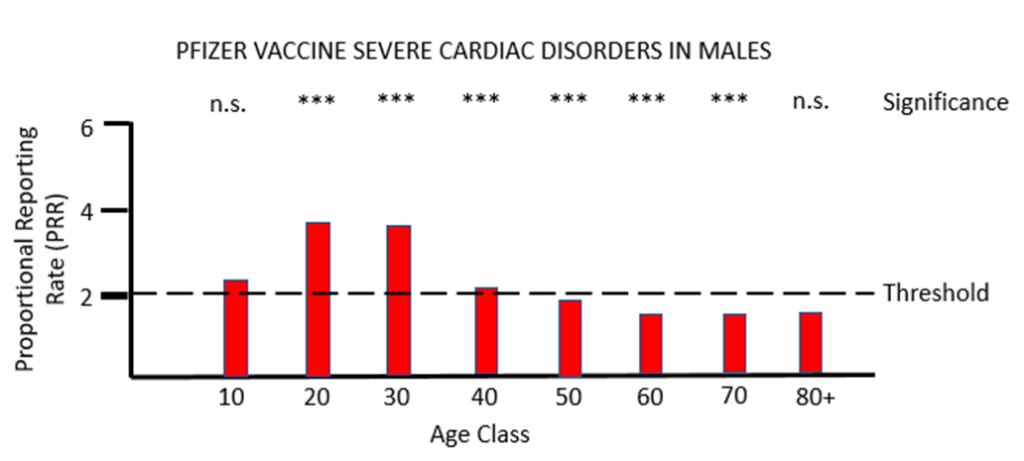
When PRR analysis is applied to investigate possible adverse effects of PF vaccination on the heart (cardiac, Figures 3a and 3b), there is a clear and significant safety signal for males between the ages of 10 and 50. For females values of PRR very close to the threshold value of 2 are present for ages 30 to 80.
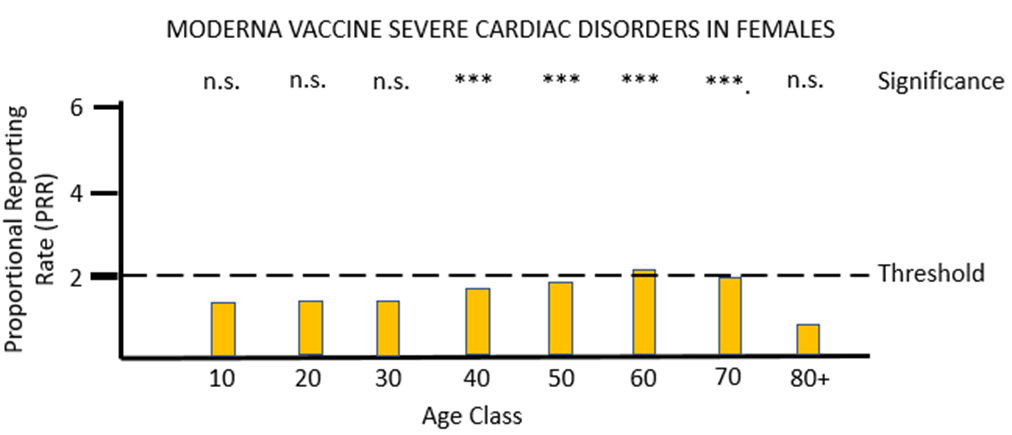
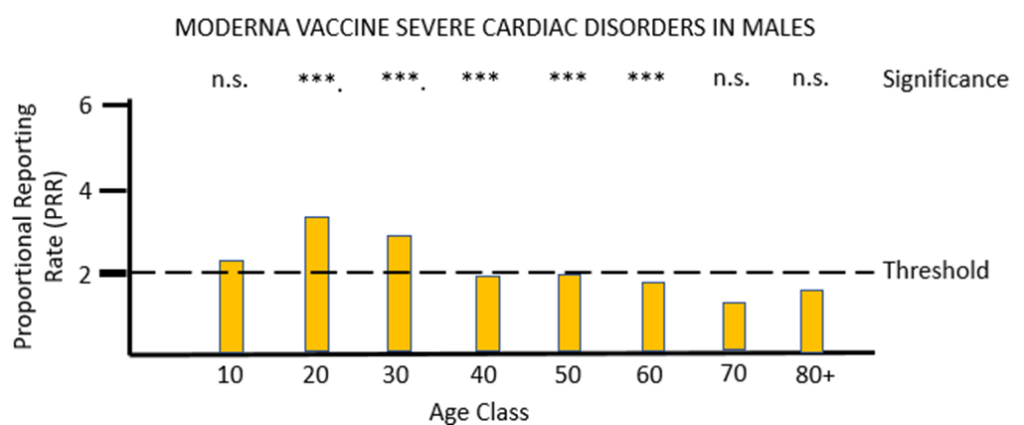
For vaccine MO (Figures 4a and 4b) the same pattern of safety signals for severe cardiac disorders are found as for PF: high and significant proportional reporting ratios in young males from 10 through 40 years of age, and reporting ratios close to or just exceeding 2 in females 50 to 80 years of age.
The MHRA has conceded in its Yellow Card summary that: “There has been a consistent pattern of higher reporting of these suspected events (myocarditis and pericarditis) with both the monovalent COVID-19 Vaccine Pfizer/BioNTech and COVID-19 Vaccine Moderna, and of these occurring more frequently in males.” However, it has not apparently made any attempt to use the Yellow Card data to demonstrate a formal safety signal in the manner described above. It is also apparently unaware of the safety signal in females. Its response to the high number of reports of myocarditis and pericarditis generated by the mRNA vaccines has not been to withdraw the offending products, but instead to alter the safety information associated with these products and alert health professionals to look out for these very serious adverse events after the relevant vaccines have been administered: “[T]he product information for both monovalent COVID-19 Vaccine Moderna and COVID-19 Vaccine Pfizer/BioNTech was updated to inform healthcare professionals and patients of these reports and provide advice to be aware of important symptoms for myocarditis and pericarditis.”
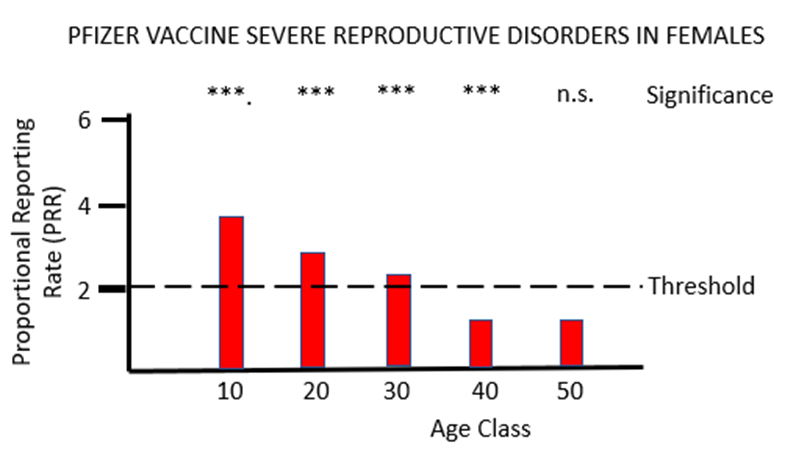
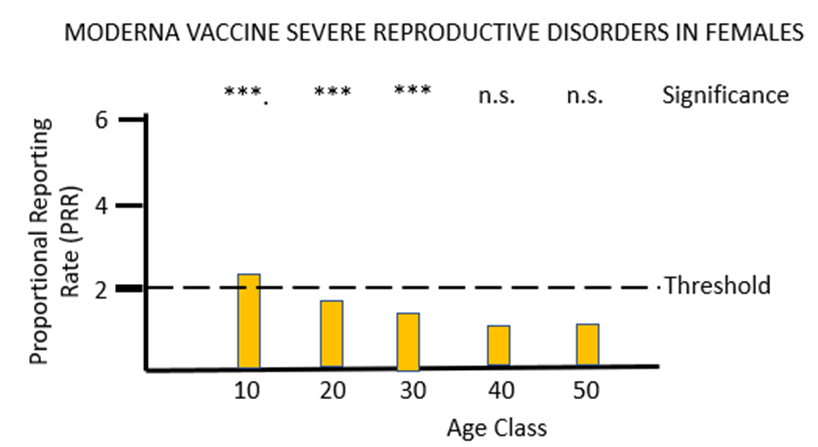
The final piece of analysis reported here investigates whether the Yellow Card data yield a safety signal associated with female reproduction following inoculation with the mRNA COVID-19 vaccines. Figures 5a and 5b illustrate the results of PRR analysis for the PF and MO vaccines respectively. For PF there are significant safety signals in age groups 10 through to 40, while for MO a formal safety signal is only found in the youngest (10 to 20 year) age groups. The vast majority of the adverse event reports for female reproduction involve disruption to the menstrual cycle and excessive menstrual bleeding. Again, these have been recognised by the MHRA as side-effects of the mRNA vaccines but their severity has been downplayed, and no attempt has been made to formally identify safety signals despite the relevant data being available. As before, the MHRA has done nothing to protect the public from the severe adverse reactions to the mRNA vaccines that the Yellow Card data have revealed: “Evidence from the most recent review suggested a possible association between the Pfizer and Moderna COVID-19 vaccines and heavy menstrual bleeding. … The product information for the Pfizer and Moderna COVID-19 vaccines is therefore being updated to add heavy menstrual bleeding as a possible side effect.”
A number of conclusions can be drawn from the analyses reported above. The first is that by applying PRR methodology it is possible to use the passively reported Yellow Card data to detect and quantify safety signals for novel vaccines, to gain insights into particular sex and age classes that may be affected by particular adverse reactions, and to compare the safety profile of different vaccines. The second conclusion is that the mRNA COVID-19 vaccines do not appear to be safe. Glaring safety signals are apparent indicating harm to the lymph system, the heart and to female reproduction. There can be no question that the mRNA vaccines should be withdrawn with immediate effect. The final conclusion is that the MHRA has provided no protection to the U.K. public from the adverse effects of the novel COVID-19 vaccines. Its regular publication “Coronavirus vaccine — summary of Yellow Card reporting” has been an exercise in defending the COVID-19 vaccines from criticism rather than defending the U.K. public from the COVID-19 vaccines. Its reports lack any scientific rigour, include not a single piece of statistical analysis to support the conclusions drawn, and are an affront to the huge number of individuals who have been injured or killed doing what they believed to be ‘the right thing’.
Dr. Richard Ennos is a retired Professor of Evolutionary Biology at Edinburgh University. He writes: “This article is dedicated to two groups within the U.K. First, the many who have been killed or injured by the rollout of the experimental and untested COVID-19 vaccines to an innocent and trusting U.K. public. Secondly to the dedicated physicians who have filed Yellow Card reports cataloguing the COVID-19 vaccine injuries and deaths. I would like you to know that your suffering and endeavours have not been in vain.”












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Is the dam about to burst at last?
I bloody well hope so!
Or this will just be a case of another silenced Dr with proof,credentials and common sense!
The thing is and as has often been the case, this doctor is retired. Most of the people who have spoken out are in the category retired/former/ex/previously.
Exactly so.
I’m guessing that as a retired/former/ex/previously, you wouldn’t stand to lose any grants or funding for speaking out and describing what you know should be obvious.
Sadly, people who are retired/former/ex/previously are often ignored, patronised or even ridiculed because they are considered out of touch and not up to date with the zeitgeist.
I think there is a tipping point with these things where the silent majority calculate that it’s better to be on the right side of the argument. We seem to be getting close to that point now with even the BBC getting in on the act.
I do hope so.
But there have been plenty of times during the past 3 years when I have thought ‘now people will see how utterly ridiculous this all is’ and nothing changes.
I will be at the protest this Saturday in London (1pm BBC headquarters). Not sure if it will make any difference.. probably won’t be reported again.
Yes, it has been a long time coming. I remember watching the vaxx propaganda change from only for the elderly and at risk in November 2020, to pushing for everyone to get it in January 2021, to the outright coercion of the vaxi pass in October 2021 – despite the first reports of ‘break-through infections’ as early as April 2021, despite the signalling of myocarditis in young men by the Israeli and US militaries in March/April 2021, the CDC’s acknowledgement thereof in June 2021, despite deaths and serious AEs from the first shots administered, despite the Israeli admission of vaxx failure when it moved on to a 3rd shot end of July 2021, despite the overwhelming infections among the 2x vaxxed and the hospitals filling with the 2x vaxxed in November 2021, despite the ongoing unexplained excess mortality since mid-2021.
Each time I thought that would be the end of the relentless pressure and coercion, but no, the b’stards just doubled down.
We have reached the tipping point, anyone who at this point has not yet moved away from the dam deserves to go under in the deluge that is to come. The next few years will be dedicated to dealing with the fall-out of the injuries, the financial repercussions and who is going to be the fall guy.
My primary concern and belief as to where the real fight lies – to ensure this never happens again and to drill it into people’s heads that constitutions and human rights treaties that clearly, uncategorically prohibited all these actions are NEVER to be trampled upon, whatever the so-called emergency. Had they been respected, we would not be looking at the economic devastation and harmed lives that we are.
I doubt it, just further and more expensive taxpayer funded activity to sweep things under the carpet. Remember WMD, Iraq, ‘grooming gangs’ MP expenses scandal, etc
What ultimately needs to happen is widespread knowledge of the discrepancy between what the public facade of the vaccines (i.e. false claims of safety and efficacy), and the reality of what is now being discovered.
Any future roll-out en masse of a new medical technology needs to be met with a healthy dose of suspicion. And mark my words, they will try this again!
Critically, the twisted, emotive justification for vaccines – “it is morally incumbent for you to take a jab, since without one you may be killing those around you” – must be relegated to the dustbin of history.
I see no reason why any medical product could be released on to the market unless it has ten, yes 10 years of safety data behind it.
And that’s not ten years of trials, that’s ten years of SAFE data, which might of course take twenty years to obtain.
My guess is that we’ll rather shortly learn that Dr Ennos must be an antisemite, a transphobe, a climate denier, an acquaintance of a guy who once knew a guy who stood next to a guy who claimed that he once saw someone reading a book written by David Icke (or even David Irving) etc, ie, the usual reaction of the woke establishment to any kind of rational criticism: A cacophony of voices screaming Evil! Evil! Evil! using some not very well made-up pretext.
One close family member has suffered life changing damage caused by the covid vaccines.
I have a number of friends who have suffered severe illness from non covid vaccines
I have no doubt that Dr Ennos is correct in his conclusions and I am most grateful to him for the work that he has done in this area.
things are so broken here it is difficult to see a solution being possible. The whole hierarchy is complicit. If you take out the top layers, then you know you have weak middle management or they would have blown the whistle. If middle mangement is the problem, then the top layers don’t have the proper controls in place. Bad, very bad.
We do need a Great Reset – just not the one that the Davos cultists have in mind.
I wish Davis was flattened with them all in it frankly. It’s a pity the god of the old testament can’t mete out some Sodom and Gomorrah treatment there.
It would indeed be extremely unfortunate if say a missile intended for Ukraine were to find its way to Davos. Some may think that would be doing humanity a favour.
I wonder if it’s crossed Putin’s mind.
More likely to be a stray Ukrainian missile
Yep. I like Bob Moran’s version, who wouldn’t? Apart from the afforementioned…
If it was up to me I would hold not only the policymakers and agencies responsible but those actually performing the injections. The information was there for all to see but they were somehow mesmerised by groupthink. People with such poor judgment should not be allowed to practice medicine.
those policy makers incentivised people to inject and the injectors went along with it. The numbers of people complicit is getting pretty big now
An outstanding piece of work by Dr Ennos who deserves our thanks for his persistence in obtaining the data.
We genuinely are looking at a crime against humanity here. Bozo, Midazolam, Raines, Jabbit, Whitty, Valance, Van Tam are just a few names springing immediately to mind who are forever damned by the murderous onslaught they unleashed on the people of this country and indirectly the world. Fishy, Chunt and Barclay will stand in the dock with them unless they ban these poisons with immediate effect.
No excuses will suffice for the hundreds, even thousands found guilty by this damning report.
I hope they burn in hell.
Never forget. Never forgive.
Completely agree. As always 😉
Thanks Jane.
Any other product in the entire history of modern medicine would have been withdrawn by this point. Yet we still have the safe and effective crowd bleating like sheep.
We need three things to happen now. Firstly remove the legal indemnity for Pfizer etc, second sue them out of existence, third destroy every political party who pushed this agenda. Won’t happen sadly.
I must say even my wonderful father in law, who is an ill man, has stopped at jab 3 after his best friend almost died.
I would argue that these gene therapies would have been withdrawn 2 years ago once evidence of harm was detected.
First rule of medicine ‘First do no harm’!
They should never have been authorised in the first place. They are novel therapies with no long term safety data.
“They are novel therapies with no long term safety data.”
Added to which there is no Short Term safety data as the Pfisser dump has proven. As other doctors have confirmed these so-called “vaccines” are not even remotely therapeutic, they are indeed bioweapons.
I thought there was some short term safety data – wasn’t it something along the lines that the vaxx sucks and was not safe?
Actually you are correct Jane. The revealed Pfisser data has confirmed that there was nothing safe about these injections from the off.
Trouble is, people come at you with the seemingly irrefutable argument that “well, if the NHS is recommending it, it must have gone through the most rigorous of safety and efficacy assessment”. But this isn’t true, is it. Firstly the regulators are under immense pressure to pass the pharma products, being as they are primarily industry-funded. Secondly, the definition of “vaccine” was changed so that these products, which would otherwise have failed the test for Emergency Use Authorization, were placed forever into the category of “vaccines” such that they could be fast-tracked for emergency use whenever required. Thirdly, those letters you get in the post stating “it’s time for your covid jab”, are not written by medical professionals, but admin people who have received the directive from their superiors. The buck stops at the MHRA, who dictate NHS activities. So Big Pharma peddles it’s products by incentivizing the regulators, who in turn dictate the policies of the health services (NHS) concerning recommending medical products to the public. Anyone who can’t see through this will spend their lives at the mercy of the pharmaceutical industry!
Glaring safety signals are apparent indicating harm to the lymph system, the heart and to female reproduction
Last week, my neighbour told me she had breast cancer. She told me that she had a good idea what to expect next week as her treatment starts as her son’s mother in law is about a month ahead of her in the treatment for her breast cancer.
And then a couple of days later, I read in the Times that Melanie Read has breast cancer, and the elephant in the room looked at me.
Someone needs to start looking at breast cancer stats.
This an extremely worrying connection. My wife was diagnosed with breast cancer in May 2022. There has been a huge upsurge in diagnoses where we live in Thailand. Until now we put it down the the fact she had missed annual check ups for three years due to Covid, but a link to the vaccines would make perfect sense. Hopefully there will be some research done to prove if there is causation rather than correlation.
Very interesting to see the data on menstrual problems. Unfortunately the ages start at 10.
Very sadly I know of two NINE year olds – yes you read that right who have started their periods. Both have been jabbed here in Thailand.
I am seeing one of the girls mother today to encourage her to make a report to Thailands pharmaco-vigilance system.
What more can I say?
I’m sure Don Joly could
debunk this ‘anti-vax’ nonsense by simply posting a pithy tweet.
Yes he can pith off ! About as funny as piles that bloke !..
To sum up, this is what I said a couple of years ago. To the credit of the local GP’s place, they haven’t bothered me at all since then. Maybe I’m on a “black list”, or whatever, but zero communication about it at all from there. W.r.t my comment in the letter: I haven’t changed my mind yet!
I ignored the two letters I received from Jab Central and put the phone down immediately when they phoned. I then told my GP not to text and offer an appointment since it was damaging my mental health 🙂 ….. and I’ve not heard a word from either Jab Central or my GP since.
I also had two letters from that place. They did not appear to have a “no thanks” option on them, so I wrote to the local Surgery directly. I never answer unknown numbers unless they leave a proper message; too many “number withheld” junk calls here. I just had an email from the Surgery within a couple of hours after sending them my notes (as shown above), and nothing more since.
Thankyou for this. I have reported several suspected vaccine complications to the MHRA, mostly Bell’s Palsy. It is a chore, but to see something changing is quite a reward.
It has been an angry 2 years for me, but I have also noticed my colleagues’ derision turn to acceptance and even praise in a few cases.
Btw, Canada as just advised people to drink less alcohol (down to 2 glasses a week! that would soak into my tongue!)
Alcohol injuries and deaths have risen because of lockdown increased drinking.
Hold the Press:- Excuse No 15, Excess deaths have been caused by excess alcohol during the lockdowns! …result
Sadly I don’t think the mRNA gravy train/bioweapon or whatever will be stopped unless and until the MSM have a sudden fit of integrity. The bloody BBC has hypnotised too many.
It seems that insofar as the covid jab is concerned the CVS damage is mainly caused by the immune system’s response to the designer spike. We have data which proves this as per the excellent article from Dr Ennos. And, we also have evidence from various papers :- See paras. 10 and 14 :-
https://www.sciencedirect.com/science/article/pii/S027869152200206X
If that wasn’t bad enough bigpharma are intending that every human on the planet receives an mRNA jab for every “disease” which they say exists. Work is already taking place and bigpharma etc are unlikely to stop.
So, we may not have to worry about a spike in the future jabs, but what further delights await?
Look at the rest of the paper for the answer to that.
The future of humanity is at stake.
Interesting article. Thank you for sharing, I hadn’t seen that one.
I have sent this article to my MP, Chris Loder ….. and utterly useless piece of CONservative lobby fodder.
He is now ignoring my emails and I don’t expect a reply to the latest one. But he won’t be able to deny receiving the information. Adopting the Ostrich position doesn’t protect ostriches.
From personal experience, people have no knowledge of the existence of the yellow card system. Whenever I mention this, people look utterly confused. They have no clue.
Last year my daughter told me about a lot of her friends having problems with their menstrual cycles. I asked if they had reported and she did not know about the yellow card system either.
The government is hiding behind the fact it is mentioned in the leaflet handed out during vaccination.
In my view a massive level of underreporting. Would be good to do a survey.
You’re right. A good friend of mine got the vaxx some time around May 2021. Some months later we were talking on the phone (due to time differences we don’t get to speak to each other that much) and mentioned that she had just heard on the radio the day before that there was a link between the vaxx and menstrual problems. She had had severe disregulation, but had not made the link before she heard it discussed.
Another friend in Spain (she did not take the vaxx) was having lunch with 3 female friends some time autumn 2021. For whatever reason, the topic of disregulated menstruation came up and all 3 then went on to tell that they all had had quite severe disregulation for months on end, yet not one had made a link to the vaxx. When my friend mentioned the link, they apparently just shrugged their shoulders and weren’t too concerned.
I’ve heard stories that women well past menopause were menstruating again – you’d expect that to have made headlines, but no.
I met with an old friend yesterday who I haven’t seen for a year. She is a self employed HR consultant working mainly in the public sector. Fully jabbed of course. She caught Covid in September of last year. And now is having a series of debilitating throat infections and colds. I have no doubt that her immune system has been damaged by the toxic jabs, but of course we are not allowed to talk about that in polite society, so once again I was confronted with the choice of keeping an old friendship that goes back 30 years or keeping my mouth shut. I chose the latter.
I’m afraid I’ve had similar experiences, yes more than one, and have also opted for the latter.
In general if friends can’t take me speaking my mind I just drop them – there’s no point in friendship if you can’t be yourself.
Lots of my opinions I am happy to leave unsaid depending on the company but the Covid madness harmed me and my family directly and continues to do so. I won’t be silent.
I have a friend whose daughter (in her twenties) works in aged care so would have had at least four vaccinations by now. The daughter is also struck down with respiratory illness that she can’t shake.
Am I being a bit stupid but I read this as having compared the PH and MO vaccines against the AZ vaccine – if I got that right, then surely comparing against all non Covid vaccines then the safety signal would be far worse?
My thoughts too, if I’ve understood it right.
Rather like comparing a 12 bore shotgun to a regular handgun, both will kill you, but one better than the other
I guess this is just meant to be a relative comparison of the dangers of the three in light of the many issues around analysing the released data. He is not going into Steve Kirsch’s (40x+) underreporting factor speculation for example, but why he is not doing this comp against traditional vaccines instead or also requires an (better) explanation.
The conclusion I draw and which he seems to draw as well is that (leaving all factors (some mentioned) aside which might increase or lower the number of truly experienced side effects compared to the hereby reported and analysed ones):
The AZ goo had almost 3x as many as such reported serious or fatal side effects than the Pfizer or Moderna goo- and the AZ goo was quietly withdrawn from ‘the market’.
But the Pfizer and the Moderna goo had even more as such reported serious side effects than the withdrawn AZ goo in the following 4 categories and to the following extent = see tables.
IMHO, still a very useful analysis and a clear and shocking result.
Reports like this are what make The Daily Sceptic worth supporting. I do hope it is read by people in authority.
Wednesday Quiz.
Rearrange the letters of the UK’s Pharmafia Bastion, the MHRA, to make another word.
Love it😂😂😂😂😂
Congratulations to the DS for publishing this article. A little piece of history perhaps.
Not peer reviewed I guess, but can this sort of material be ignored much longer? I think not.
Technical point, if I’ve understood it properly. I thought the Moderna stab was effectively about 3 times as much mRNA – so I wonder why the adverse event signals (PRRs) are generally significantly lower?
A great piece, I do hope someone somewhere with a bit of authority and nous gets to read this and comprehend what it is saying.
I have a slight problem with certain terminology I notice being used in these types of feature…
They refer to “Safety Signals”. Isn’t that a bit misleading or is it just me? Surely the correct termonology should be “Danger Signals”. Matbe I’m just being pedantic.
https://www.ukcolumn.org/blogs/it-is-time-to-stand-up-to-those-who-contort-the-meaning-of-antisemitism
The brilliant Iain Davis over at UK Column News lending his support to Andrew Bridgen. Along the way he utterly destroys Fishy and Midazolam. And that in itself is a very, very sad indictment of the moral vacuums which these two sad specimens represent.
Very much worth reading in full.
“International Holocaust Remembrance Day –
was established by the United Nations to “honor the victims of Nazism”. Those who flagrantly abuse the intended meaning of the term antisemitism do nothing but dishonour those victims. They should be thoroughly ashamed of their conduct—but that would require some intellectual honesty and a sense of morality on their part. Do they possess either?”
The article is sort-of worth a read. But in the context of the Bridgen cause, it’s just more noise. The people who want to silence Bridgen want a noisy and emotive discussion of antisemitism and Holocaust in order to bury a discussion about the covax-injured and covax-side effects. That the accusations against Bridgen are laughable accomplishes this very nicely.
This is the line that got me:
‘…that the enormous efforts of those who have submitted Yellow Card reports of COVID-19 vaccine adverse effects have not been in vain.’
We can add this to the MHRA’s already extensive list of crimes. Even when people were brave enough to report their injuries, the MHRA found every way possible to diminish, ignore, gaslight and hide them.
These people must be dealt with. Why isn’t June Raine in prison?
How much of MHRA’s funding is from Pharma? 90%, did I hear?
Doubt it very much. They’ve come this far…
This is exactly what happens when the CEO of the MHRA arrogantly decides that the regulator will become an enabler. June Raine should be sacked but she won’t be as that would cause too many other bureaucrats to be removed as well.
Very grateful for the doctor’s publication but it needs practicing doctors to speak out not retired ones. More doctors like Steve James who challenged Savid Javid are the ones who demonstrate moral courage, fearlessness, observe the highest ethics of a practicing doctor with the result of making real change. There would have been mandatory vaccination of all NHS staff but for this hero.
This should be helpful to Andrew Bridgen in his defamation action against Matt Hancock for saying that AB’s comment was a ‘disgusting, anti-semitic, anti-vax, conspiracy theory’.
interesting (and pretty damning) article. In the interests of accuracy, there is one small error though. The article says:
“All three vaccines rely on novel technology that has never before been used in humans.”
In fact the adenovirus vector technology used by the AstraZeneca vaccine has been used before, in a vaccine for Ebola.
Sorry to be a bit dim, but could someone explain how the following statements are reconciled?
From paragraph 8 above:
‘A cursory look at the C-19VYC data indicates that the rate of reporting of serious and fatal adverse events is nearly three times higher for the adenovirus AZ vaccine (3.912 serious or fatal reaction reports per 1,000 doses) than for either of the mRNA vaccines PF or MO (1.341 and 1.344 serious or fatal reaction reports per 1,000 doses respectively).’
From paragraph 14 above:
‘It should be noted that when the analysis is conducted in the manner described, it yields minimum estimates of the strength of the safety signals because it assumes that the AZ vaccine does not increase the rate of the adverse reaction being studied.’