
On December 1st, the U.K. Government published a technical report on the Covid pandemic.

We commented on it in our post and its late pick-up by the mainstream media and their lack of critical approach to its ‘independent’ content.
One of the paragraphs that interested us is the one in which the Chief Medical Officer explained the non-Covid related excess mortality most European nations are experiencing:
There is little doubt that delays in presentation, reductions in secondary prevention (such as statins and antihypertensives) and postponement of elective and semi-elective care and screening will have led to later and more severe presentation of non-Covid illness both during and after the first three waves. The combined effect of this will likely lead to a prolonged period of non-Covid excess mortality and morbidity after the worst period of the pandemic is over.
There can be little doubt that blocking access to, say, cancer screening and treatment will have disastrous consequences – one of the many legacies of lockdowns. But how did Professor Whitty and his team conclude that excess cardiovascular mortality was due to a lack of statins and antihypertensives?
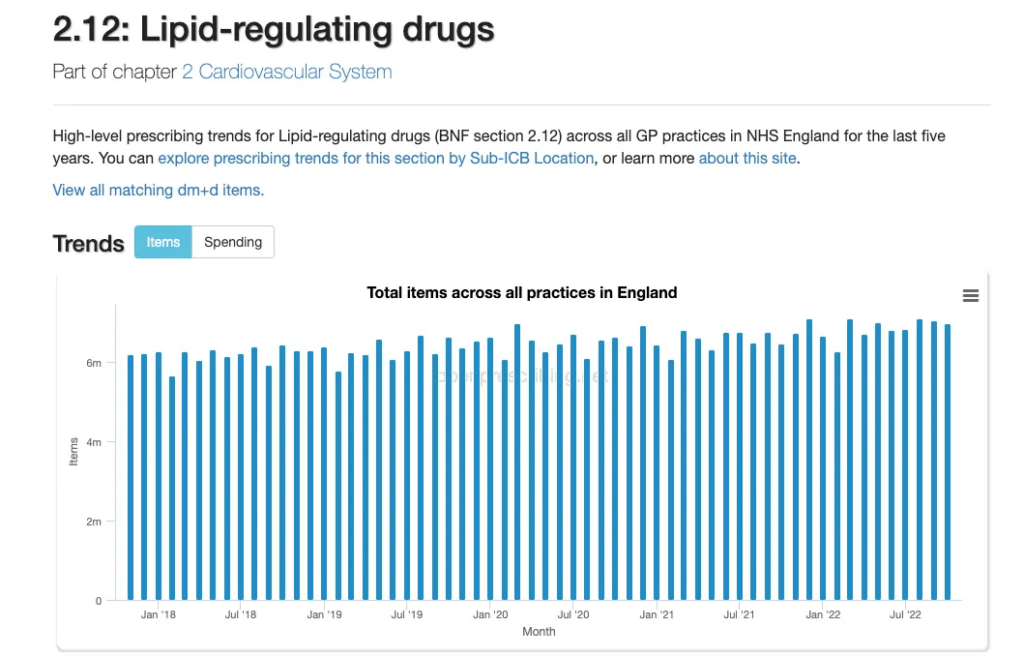
Primary care is where the bulk of statins and antihypertensives are prescribed, but did the prescriptions of such drugs change during the pandemic?
Not according to Open Prescribing, which is based on monthly NHS prescribing data.
Another aspect that needs to be considered when looking at whether a lack of statins could have caused a sudden increase in cardiovascular deaths is the length of time of exposure to the drugs.
A large meta-analysis of the effects of statin use in primary prevention compared to placebo reported a number-needed-to-treat (NNT) of 138 people with statins for five years to prevent one death, 49 to prevent one cardiovascular disease (CVD) event, and 155 to prevent one stroke.
The figures for secondary prevention (in those who have known heart disease or a history of stroke) are better, as you would expect: NNT of 83 for one death after five years of exposure to a statin.
The five years do not fit the introduction of restrictions in March 2020, nor is there any evidence that lipid regulating and antihypertensive drugs were prescribed less in the last three years based on the NHS’s data.
There is evidence of a fundamental change in working practice and primary care delivery during the three periods of restrictions. Six measures recovered to pre-pandemic levels within a year, asthma and COPD (pulmonary disease) reviews recovered by August 2021, and blood pressure monitoring and cardiovascular disease risk assessment had a sustained drop in activity up to December 2021.
However, a sustained drop in monitoring is unlikely to be the reason for the increase in excess deaths. In 2017 we did a systematic review of the effect of global cardiovascular risk assessment in adults. We found its use did not translate into reductions in CVD morbidity or mortality.
So what might be the cause? The British Heart Foundation considers “severe ambulance delays, inaccessible care and ever-growing waiting lists are contributing to heart patients dying needlessly”.
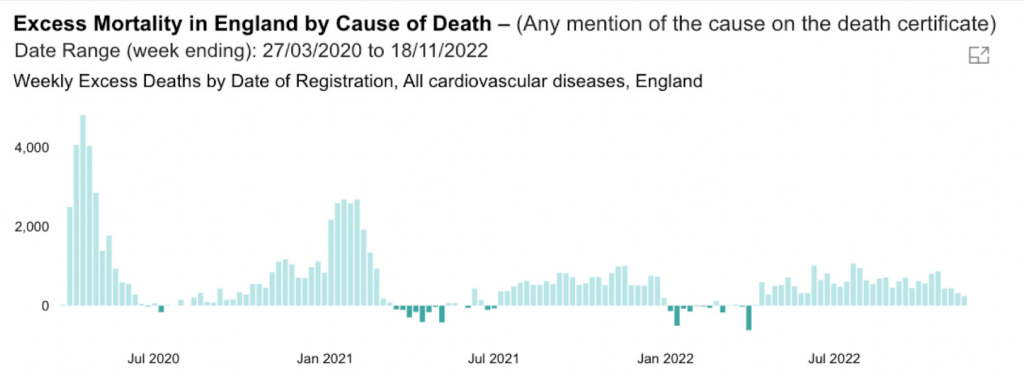
While the data from the Office for Health Improvement and Disparities report an excess of cardiovascular disease mortality, the ‘independent’ report produced by the U.K. Government does not attempt to understand what is causing the excess mortality from CVD.
In the last year, there has been an excess of 21,841 deaths with CVD mentioned on the death certificate. Our analysis suggests it isn’t a fall in drug treatment, and the drop in CVD risk monitoring can’t account for it, given the lack of evidence of an effect.
Given all its resources, the Government could and should do better to get to the bottom of what is driving the excess in cardiovascular deaths. We’ll keep digging.
Dr. Carl Heneghan is the Oxford Professor of Evidence Based Medicine and Dr. Tom Jefferson is an epidemiologist based in Rome who works with Professor Heneghan on the Cochrane Collaboration. This article was first published on their Substack blog, Trust The Evidence, which you can subscribe to here.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
The inference of this article is obvious, the elephant in the room.
Does that mean the excess cardiovascular deaths were not caused by climate change???!!!
From Bob Moran …
Lancet is blaming SADS on air pollution 🙂
(November 2022). https://bgr.com/science/study-claims-tiny-particles-in-the-air-can-cause-sudden-heart-attacks/
Clown world. Nothing to do with poison injections.
They think we are as idiotic as they are
Sceptic readers not but most of the population most definitely are unfortunately which is why they get away with the cr4p.
‘Nobody is blinder than the person who decides he does not want to see’
Dot to dot should be on the curriculum not enhanced maths
Bob Moran is a genius. He never fails to prove that a picture can say a thousand words.
That’s next week.
The guilty keep lying. One day, maybe soon maybe not so soon, they will run out of lies, or they will end up telling lies so big that even the sheeple will cotton on.
One can but live in hope!!!
“the Government could and should do better to get to the bottom of what is driving the excess in cardiovascular deaths. We’ll keep digging.”
Hilarious. Yes keep digging Carl, right underneath the giant Syringe shaped elephant. Maybe you’ll get to Australia and you can ask them what caused it.
Don’t look here……………………………………….look over here…
Carl,
You gaslight on plenty of TV and Radio shows. Regularly. Weekly in fact.
You know what is causing this just as much as I do – and I’m not a medical professional.
Why not compile the facts as you have them now and come out on TV and say there is strong indication/evidence that the excess deaths are caused by…….
…or will you keep the TV and Radio slots for as long as you can, not mention the unmentionable while the rest of us guess the correct answer and ask why all these super-experienced and super-educated medical professionals continue to be “baffled”.
There is real harm in the public being caused because of loss of confidence (more than now) in the medical profession because you/they will not call out the Emperors new clothes. We all see the nakedness.
Slowly slowly catchy monkey.
It’s a bit harsh to criticise a practitioner of ‘evidence based medicine’ for not resorting to speculation. CH and team are asking the government to provide the evidence required to form conclusions and then scrutinise that which is provided to test its reliability, that’s the difference between him and Dr Malhotra or Dr McCullough (neither of whom i’m criticising either, they just take a different approach).
I want to see these jabs exposed just as much as the next guy but it won’t be done by wild speculation.
I’d say we’re a bit past “speculation” at this point. It’s probably because he doesn’t want to risk jeopardising his job. Understandable but a shame because he, along with the likes of Malhotra, would have a heck of a lot of clout. No offence to Prof Heneghan but it does come off as cowardice. Don’t tell me he isn’t personally seeing evidence of vax harms first hand in his clinical practice. He’d also be in a position to establish the vax status of his patients.
I quite agree. We’re 2 years in. The time for speculation is long gone. Enough data the world over has been collected. The Prof has a duty of care both clinically and academically. It’s painfully obvious he’s dancing around the flaming obvious, all the while ignoring the Yellow Card system screaming the safety signal for anyone with zero letters behind their name to see. He’s failed in his duty to protect patients and inform the public and that’s a huge disappointment for someone so highly credentialed. He’d make one hell of an opponent for tptb and ally for others who’ve got the courage to speak up though. What a let down.
Swineflu Vaccine:- 1 adverse reaction in 100,000. Withdrawn
Rotashield Vaccine:- 20 adverse reactions in 100,000. Withdrawn
Covid mRNA Vaccine:- 125 adverse reactions in 100,000. Actively promoted.
(yet the AZ C19 Vaccine was quietly withdrawn with (less than??) 1/800 reaction rate)
Adverse reaction reporting is reputed to be only 1/10 of actual events?
That I would suggest is a very good starting point for any evidence based scientist and the medical profession to openly question the current “treatment” plan.
We all need to keep an open mind until there is clear evidence one way or another.
Those who claim the vaccines are causing many of the excess deaths need to explain why there haven’t been excess deaths in the highly vaccinated Nordic countries, at least up until July 2022:
“Between January 2020 and July 2022, Sweden’s age-standardised mortality rate was 4% lower than the five-year average. By contrast, Iceland’s was 3.9% lower, Denmark’s was 2.8% lower and Finland’s was 1.7% lower.”
https://dailysceptic.org/2023/01/04/sweden-did-better-than-its-neighbours/
Cholesterol…statins …a whole other can of worms…..40 million Americans are taking statins!
‘Our review of the literature indicates that statin therapy for both primary and secondary prevention of CVD is not warranted for individuals on an LCD with elevated LDL-C who have achieved a low triglyceride/HDL ratio.’
‘….a person on an LCD with a nonatherogenic lipid profile (low TGs/high HDL-C) is more likely to experience the adverse effects of statins including an increased risk of new onset type 2 diabetes, an increase in fasting blood glucose in patients with and without diabetes, mitochondrial dysfunction, tendinopathy, myopathy, acute kidney injury/renal failure and cognitive deficits than benefits.
https://journals.lww.com/co-endocrinology/Fulltext/2022/10000/Statin_therapy_is_not_warranted_for_a_person_with.14.aspx
Cognitive deficits?
‘……the study predicts that the number of people with dementia will go up in every country in the world, resulting in a near tripling in the global rate of dementia.’
https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(21)00249-8/fulltext
Hmmm………
Great points Monro, and completely echoes what a long career in medicine has taught me.
A simple test of lipid subfractions (which splits LDL into 7 subtypes of which only some are atherogenic) as well as HDL and TG’s can stratify who may benefit from statins.
In my experience, few GP’s know of this test, such is the power of Big Pharma marketing.
The deleterious effects of the mRNA spike protein on the cardiovascular vascular system were theorised years ago – Sucharit Bhakdi – and on a biomolecular level this paper, particularly para. 10 :-
https://www.sciencedirect.com/science/article/pii/S027869152200206X
No doubt those to be tasked, lol, with looking at any causal relationship will be well aware of the above.
Maybe I’m stupid, but to my mind we have –
Excess deaths from CVE’s in highly vaxxed countries,
A temporal link with the mRNA vaccines,
Evidence of harmful effects on the immune system/CV system theorised in many papers written by independent experts in their appropriate fields and absence of any coherent rebuttal.
Instead all we do have is a deafening silence from the public face of the medical profession, government and the MSM.
Warning for the jabbed, CVE’s may just be the start of the problems. But no worries, those won’t be investigated either.
CVE’s may just be the start of the problems. But no worries, those won’t be investigated either.
Indeed. It makes me shudder, and I’m unstabbed.
Apologies, ref to above paper should have been to para 14 in as opposed to just para 10
Considering he’s Prof of Evidence Based Medicine, Dr Heneghan sure is reticent about mentioning the word “vaccine”. It’s always the same in his articles. Weird..
The usual suspects would like us to believe that it is. It would support the finances of the manufacturers. As one or two have mentioned Malhotra in their comments, it’s worth noting that he has his own point of view about the large scale use of statins.
Aseem Malhotra is not alone in his view of statins. The International Network of Statin Skeptics has thoroughly trashed the cholesterol/heart disease link but has faced the same stonewalling and denigration that coronavirus vaccine sceptics are now seeing. Statins do reduce cardiac risk, but only a tiny bit, and the effect is almost certainly because of an anti-inflammatory action and not anything to do with their cholesterol-lowering properties – look at the recent introductions which are even better at cholesterol-lowering but no better at reducing cardiac risk. So I think that blaming a (non-existent) reduction in statin prescriptions is ridiculous. As far as being over-cautious with blaming vaccines goes, I think this is wise, as the high vaccination levels run in parallel with the appearance of new virus variants such as Omicron, and it is far from clear yet whether the viral variants confer a differential cardiac risk. It’s also pointed out that the risk of inflammatory cardiac disease is still (probably) higher with infection than with vaccine. Nonetheless it makes more scientific sense to pause the vaccination programme while all of this is sorted than continue, at risk, until the evidence is totally clear-cut.
Dr John Campbell with an inmteresting video on the subject.
https://www.youtube.com/watch?v=26zP0YhEdmg
All these heart attacks are due to anything and everything but the real cause – which we all know.
We need to start laughing at the professional liars in Public Health when they come out with such ridiculous statements.
Trying to argue with professional liars using facts doesn’t gain traction. Laughing at them will.
Not listing vaccines as a hypothetical cause to be investigated and quantified alongside e.g. ambulance delays, is in itself suspicious.